


This issue brief is the second of a two-part series examining the behavioral health workforce shortage in Kansas. It describes the age and geographic distribution of a large segment of the Kansas behavioral health workforce, as well as strategies to reduce the workforce shortage. The first brief, Defining the Behavioral Health Workforce in Kansas, describes the types, training, licensure and quantity of certain behavioral health providers in the state. An earlier series of issue briefs examined the primary care workforce shortage, and the age and geographic distribution of primary care physicians in Kansas.
Addressing Behavioral Health Workforce Needs in Kansas
11 Min Read
Dec 20, 2022
By
Cynthia Snyder, M.A.,Angela S Wu, M.S.,
Hina B. Shah, M.P.H.,
Wen-Chieh Lin, Ph.D.
Key Points
- Most psychiatrists and licensed specialist clinical social workers (LSCSW) are located in urban areas. The population per psychiatrist is 7,614:1 for urban/semi-urban areas and 42,022:1 for rural areas. The population per LSCSW is 2,132:1 for urban/semi-urban areas and 5,816:1 for rural areas.
- An estimated one-fourth (24.7 percent) of psychiatrists and one-fifth (20.9 percent) of LSCSWs are age 65 or older. National models predict a constricting workforce as retirees leaving the profession outpace new professionals entering the field.
- Telehealth can address challenges in rural service delivery including provider shortages and distance to care.
- Kansas has opportunities to increase the prescribing workforce. Growing professions of physician assistants and advance practice registered nurses, as well as retention of psychiatric residents, will all have a positive impact on behavioral health workforce growth.
Introduction
In Kansas, many practitioners provide behavioral health services, including prescribers, independent practice behavioral health professionals and other behavioral health professionals.
Prescribers include psychiatrists, who are supported by physician assistants (PA) and advance practice registered nurses (APRN), all of whom are able to prescribe medicine. Psychiatrists comprise two-thirds (68.2 percent) of the prescribing workforce.
Other behavioral health professionals include psychologists, social workers, addiction counselors, marriage and family therapists, professional counselors and mental health technicians. Of the subset of those behavioral health professionals who can practice independently, licensed specialist clinical social workers (LSCSW) comprise almost one half (47.3 percent).
This issue brief profiles psychiatrists, who comprise the largest segment of the prescriber workforce, and LSCSWs, who comprise the largest segment of the non-prescribing independent practice behavioral health workforce.
The estimates described in this brief are based on licensing data available from the state. The psychiatrists discussed are physically located in Kansas and provide at least some outpatient behavioral health services. The LSCSWs discussed have an active license, are physically located in Kansas, and working at least 10 hours a week and 30 weeks a year. A small number of LSCSWs practice in more than one region and, for geographic analysis, they were distributed proportionally to their time at each site.
Geographic Distribution
The distribution of behavioral health providers across Kansas is important because it impacts the ability of the community to access needed services. Most Kansas counties have a shortage of behavioral health providers and in four regions, the shortage is pronounced. The uneven distribution of the workforce accentuates the challenges of rural areas, not only in workforce, but also in access, availability of affordable services and stigma.
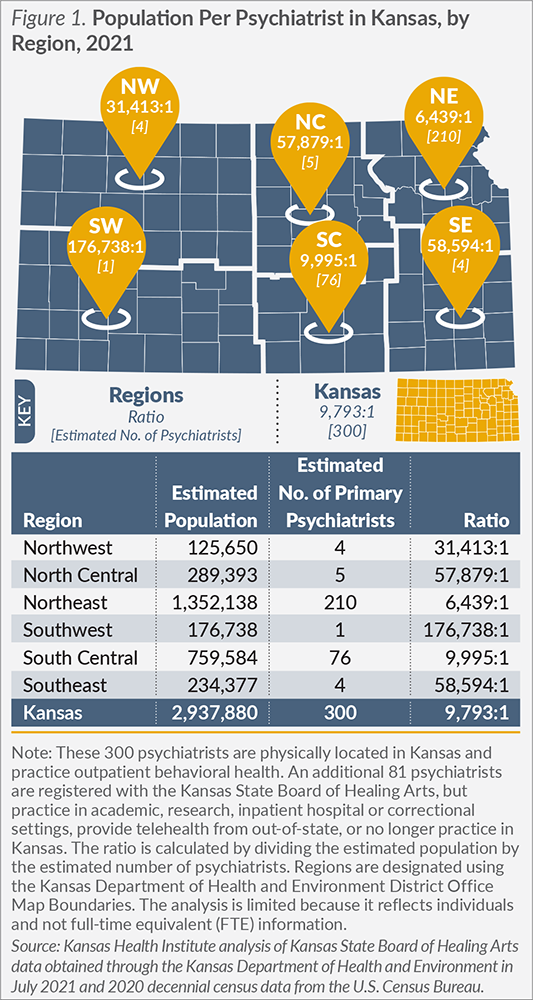
The state has one psychiatrist for every 9,793 Kansans. However, the overwhelming majority of psychiatrists (93.7 percent, 281 out of 300) are physically located in an urban/semi-urban setting. Prior to COVID-19, some psychiatrists traveled to rural areas to provide in-person services on a limited basis. Now, many of those services are being provided through telehealth. The geographic distribution of psychiatrists across Kansas (Figure 1) reflects the rurality of the four regions that have five or fewer psychiatrists per region. Even with semi-urban counties within these regions, such as Saline County (City of Salina), the availability of psychiatrists is limited. This underscores the significant challenges rural areas face in attracting and retaining psychiatrists.
Southwest Kansas has the fewest psychiatrists. One psychiatrist is physically located in the region to serve 176,738 Kansans, according to Kansas licensure data. The psychiatric needs of this region are also addressed through one psychiatric advance practice registered nurse (APRN), one Kansas-based telehealth provider and two out-of-state telehealth providers. Southwest Kansas illustrates how uneven the distribution is across regions and how rural areas are trying to meet their workforce needs.
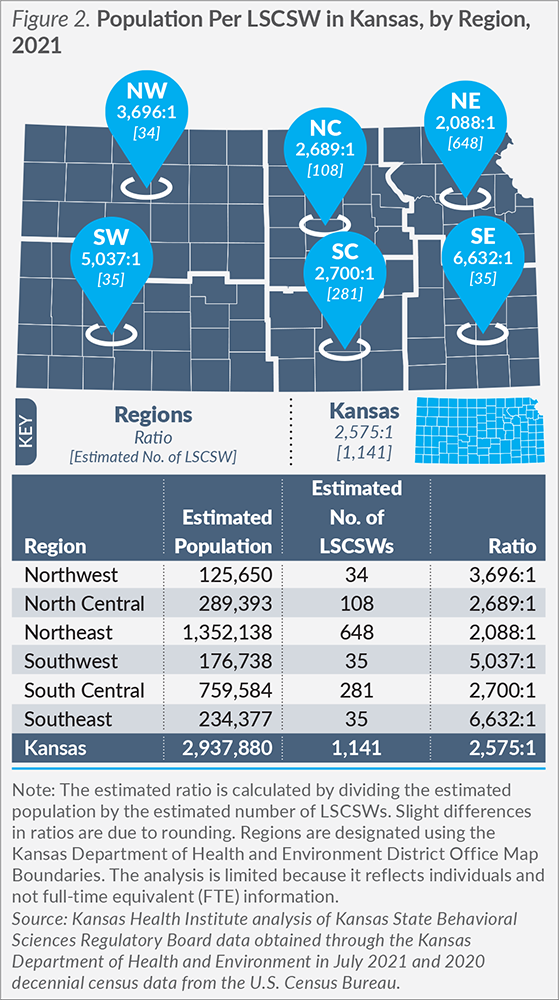
There are 1,141 practicing LSCSWs reporting a Kansas physical address, or one LSCSW for every 2,575 Kansans. As with psychiatrists, the majority of LSCSWs are located in an urban/semi-urban setting, but the difference is not as stark. There are 1,004 (88.0 percent) LSCSWs located in urban areas and 137 (12.0 percent) located in rural parts of Kansas.
Northeast Kansas has the most favorable ratio, with one LSCSW for every 2,088 Kansans in the region, and over one-half (56.8 percent, 648 out of 1,141) of LSCSWs in the state. Figure 2 highlights the geographic distribution of LSCSWs across the state, including regions with very limited numbers of LSCSWs.
Age and Retirement
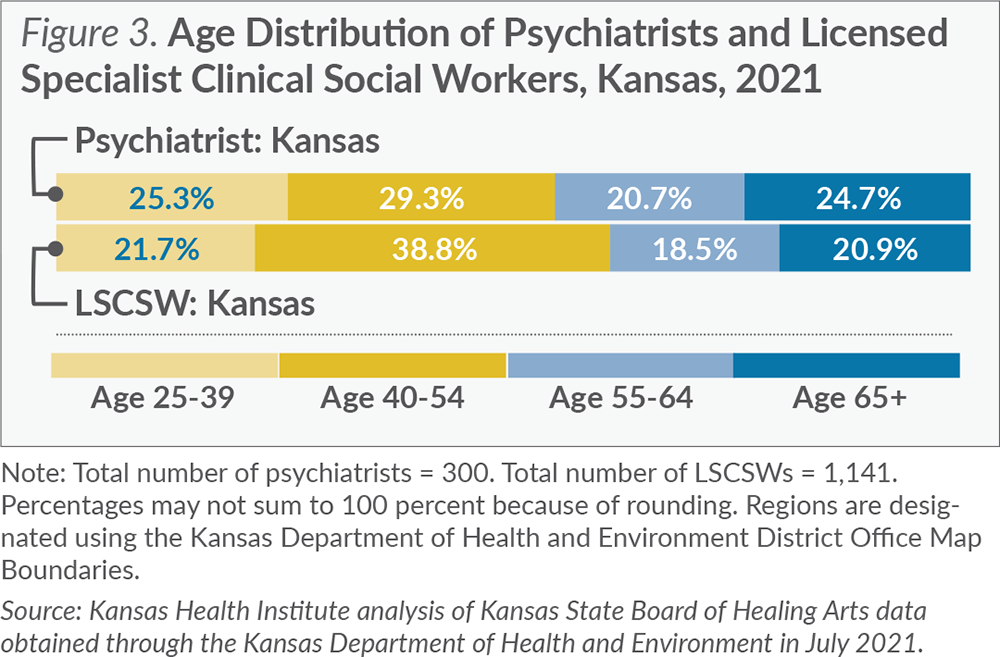
An aging workforce can signal reduced hours worked and impending retirement. The average age of a psychiatrist is 53; for an LSCSW, the average age is 51. In Kansas, almost one-half (45.4 percent) of the psychiatric workforce is over the age of 55 and potentially within 10 years of retirement. LSCSWs have a similar trend with 39.4 percent over the age of 55, but with a slightly smaller proportion of the workforce over age 65. Figure 3 focuses on the age distribution and highlights the workforce over the age of 55.
Despite the high proportion of psychiatrists over the age of 55 in Kansas, the proportion is lower than the national average. The Association of American Medical Colleges tracks physician demographics by specialty. The most recent workforce report shows nearly two-thirds (61.3 percent) of psychiatrists nationwide are over the age of 55. National models that predict long-term trends in the psychiatric workforce estimate a contracting workforce as psychiatrists retire.
As more of the workforce retires, new providers are needed to enter the profession to maintain the behavioral health workforce and address workforce shortages.
Strategies to Address Workforce Shortages
Reduce Health Disparities
Acknowledging the importance of the social determinants of health, communicating in a culturally competent way and reducing stigma are powerful tools in improving the health of historically underserved populations.
Integrating cultural humility curricula into the education of health professionals and creating a diverse workforce are key strategies to reducing health disparities.
Promising practices to improve workforce diversity and cultural humility include programs that increase interest in health careers, particularly among people from racial and ethnic minority groups, and programs that provide mentors, increase skills and prepare students for higher education. Kansas workforce promotion strategies include establishing programs that promote interest in behavioral health careers in adolescents.
A diverse workforce in race, ethnicity and other characteristics supports access to care and greater patient satisfaction with concordance of behavioral health care providers and patients. Race and ethnicity data are collected, but are not required fields. Consistent collection is needed to accurately describe diversity within the workforce.
A recent study by the National Association of Social Workers highlights the importance of early support in the career paths of behavioral health professionals. Of 2019 Master of Social Work graduates, 46 percent were the first members of their family to graduate from college. This was especially true for Hispanic/Latino (73 percent) and Black/African American (57 percent) graduates.
Grow-Your-Own Approach
The Strategic Framework for Modernizing the Kansas Behavioral Health System includes a number of high priority workforce recommendations, including the development of a long-term workforce investment plan emphasizing the “grow-your-own” approach.
For psychiatry, the grow-your-own approach includes not only the career path through medical school and residency, but also retaining new psychiatrists. The University of Kansas School of Medicine campuses in Kansas City and Wichita have psychiatric residency programs. Residency program information is not currently available in Kansas State Board of Healing Arts data, but medical school information is available. Psychiatrists graduating from the University of Kansas School of Medicine comprise 22.0 percent of the workforce, while 18.0 percent are from neighboring state programs and 60.0 percent are from other state or international programs.
Nationally 56.0 percent of psychiatrists, more than any other specialty, practice in the state where they completed their residency. In the neighboring state of Nebraska, the most recent behavioral health workforce report highlights retaining 9 of 11 psychiatry residents. Adding additional residency spots and retaining residents are proven methods to increase psychiatrists within the state.
Telehealth
Telehealth provides an opportunity to increase access to the behavioral health workforce, including those practicing from out of state. Telehealth also increases training opportunities and improves retention statewide through reduced professional isolation. While telehealth was growing prior to COVID-19, it has expanded rapidly as an opportunity to deliver care to patients in their homes and limit transmission of the novel coronavirus. Nearly all psychiatrists in Kansas now offer telehealth services.
Under the Kansas Telemedicine Act, for the length of the public health emergency, telehealth services are reimbursed at the rate of covered services provided in an office setting. The future of telehealth will be strongly influenced by reimbursement models, access to infrastructure funds and licensing requirements for out-of-state providers. Other legislation such as the Psychology Interjurisdictional Compact (PSYPACT) allows licensed psychologists from other compact states to practice in Kansas through telehealth services. While there are many benefits of telemedicine, continuity of care, privacy concerns, expense and access to technology, as well as a patient’s technology capabilities, are all concerns.
Integrated Care
Integrated care is the collaboration between behavioral health professionals and medical clinicians to provide complete treatment and improve overall health. Integrated care happens on a continuum from basic collaboration and co-located care to fully integrated care. While all providers consider the physical and mental health of patients, several organizations are moving toward fully integrated services, which includes both medical and behavioral health services. Fully integrated care engages medical providers in addressing gaps in behavioral health services.
Lessons Learned
Nebraska’s behavioral health workforce has seen positive growth since 2010, largely due to an increase in the number of independent practice behavioral health professionals. While the number of psychiatrists in Nebraska is down 5.6 percent in the timeframe between 2010 and 2018, the overall prescriber workforce has increased by 17.3 percent with increases in both psychiatric APRNs and psychiatric PAs. Workforce trends, geographic distribution and workforce characteristics are tracked biennially by the Behavioral Health Education Center of Nebraska (BHECN). BHECN presented its strategies to the 2021 Special Committee on Kansas Mental Health Modernization and Reform. Strategies included:
• Engage and Recruit — the Ambassador Program connects students in underserved areas with resources and mentors to increase interest in behavioral health professions. BHECN produced and distributed 10,000 copies of Pathways to a Career in Behavioral Health.
• Prepare and Train — BHECN supports placing student trainees into internship and training programs with an emphasis on opportunities in rural and underserved communities.
• Retain and Support — BHECN supports the current behavioral health workforce through professional development, training opportunities and resources.
Conclusion
The aging and geographically clustered behavioral health workforce in Kansas highlights the need to innovate and prepare for future needs, especially in rural areas. Kansas is in a position to leverage existing training programs and workforce to meet current and future behavioral health needs of Kansans. Along with other states that have expanded their behavioral health workforce, Kansas can track trends over time, examine and address barriers, and ensure that strategies to increase workforce are successful.
About Kansas Health Institute
The Kansas Health Institute supports effective policymaking through nonpartisan research, education and engagement. KHI believes evidence-based information, objective analysis and civil dialogue enable policy leaders to be champions for a healthier Kansas. Established in 1995 with a multiyear grant from the Kansas Health Foundation, KHI is a nonprofit, nonpartisan educational organization based in Topeka.